| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website https://gr.elmerpub.com |
Original Article
Volume 19, Number 2, April 2026, pages 74-84

A Supervised, Online, Home-Based Eccentric Resistance Exercise Program for Patients With Metabolic Dysfunction-Associated Steatotic Liver Disease
Kedar S. Deshpandea, g, Kazunori Nosakaa, Aus Molanb, Isaac S. Rajc, John K. Olynykd, e, Oyekoya T. Ayonrinded, e, f
aExercise Medicine Research Institute, School of Medical and Health Sciences, Edith Cowan University, Perth, Australia
bPathwest Laboratory Medicine, Perth, Australia
cSchool of Allied Health Sciences, Charles Darwin University, Darwin, Australia
dCurtin Medical Research Institute, Curtin University, Perth, Australia
eDepartment of Gastroenterology and Hepatology, Fiona Stanley Hospital, Perth, Australia
fMedical School, University of Western Australia, Perth, Australia
gCorresponding Author: Kedar Deshpande, Exercise Medicine Research Institute, School of Medical and Health Sciences, Edith Cowan University, Perth, Australia
Manuscript submitted February 2, 2026, accepted April 6, 2026, published online April 27, 2026
Short title: Exercise Program for Patients With MASLD
doi: https://doi.org/10.14740/gr2131
| Abstract | ▴Top |
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most common non-communicable chronic liver disease worldwide, increasing long-term risk of cirrhosis, type 2 diabetes mellitus, and cardiovascular diseases. Although reducing liver steatosis by increasing physical activity can lower these risks, patients with MASLD often struggle to exercise regularly. We examined the effects of a supervised, home-based, online bodyweight eccentric exercise program on liver and metabolic markers, and physical fitness in patients with MASLD.
Methods: Sixteen adults with MASLD (24–91 years) were assigned to an exercise group (n = 9) or a control group receiving lifestyle counselling (n = 7). The exercise group participants performed an online progressive bodyweight eccentric exercise program targeting trunk, leg, and arm muscles for 5 to 25 min per session, 5 days a week, for 8 weeks. Outcome measures included severity of hepatic steatosis (controlled attenuation parameter (CAP)), anthropometric measures (waist and hip circumferences), liver enzymes, and physical function tests, which were assessed at baseline and after the 8-week period.
Results: All participants in the exercise group completed 40 exercise sessions, and showed reductions in CAP (−13.2±13.8%, P = 0.03), waist circumference (−4.4±13.5%, P = 0.007), hip circumference (−2.6±11.1%, P = 0.03), and serum gamma-glutamyl transferase (−23.9±30.0%, P = 0.03), which were not evident in the control group. Physical fitness of the exercise group participants improved, including the sit-to-stand (24.3±33.2%, P = 0.03), 3-m timed up and go (−15.6±16.4%, P = 0.01), 2-min step test (37.5±20.5%, P = 0.008), and single-leg balance (25.1±37.6%, P = 0.04).
Conclusion: The exercise program was effective in reducing hepatic steatosis and increase physical fitness in patients with MASLD, highlighting the efficacy of the home-based eccentric exercise program in enhancing liver and metabolic health.
Keywords: Controlled attenuation parameter; Liver stiffness; Liver enzyme; Lipid profile; Physical function test; Exercise adherence
| Introduction | ▴Top |
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD) [1], is the most common non-communicable chronic liver disease, affecting approximately 30% of the adult population worldwide [2]. The hallmark of MASLD is the accumulation of triglycerides (TG) in at least 5% of hepatocytes, along with at least one metabolic dysfunction feature, excluding secondary causes such as excessive alcohol intake. MASLD encompasses a range of liver pathologies, from simple steatosis to metabolic dysfunction-associated steatohepatitis (MASH), progressing through varying severities of liver fibrosis to cirrhosis or hepatocellular carcinoma [3]. MASLD is one of the most common causes of chronic liver disease, but it is often underappreciated as a cause of cirrhosis [4].
The global burden of MASLD is substantial, with an estimated 38% of adults and 7–14% of children and adolescents currently affected worldwide, and adult prevalence projected to exceed 55% by 2040, contributing to a rising incidence of advanced liver disease and MASLD-related deaths [5, 6]. Among individuals with type 2 diabetes mellitus (T2DM), MASLD prevalence is estimated to be between 55% and 70% [7]. MASLD is associated with a two-fold increased risk of developing T2DM and cardiovascular disease [8, 9]. However, reversal of hepatic steatosis is associated with a reduced likelihood of developing these [10, 11].
Lifestyle modifications, including dietary changes and regular exercise, remain the cornerstone of MASLD treatment [12]. Both aerobic and resistance exercises have demonstrated benefits for liver enzymes, liver fat, and metabolic risk factors [13, 14]. Despite increasing evidence supporting these benefits, the optimal type, duration, intensity, and frequency of exercise for MASLD management remain unclear. Furthermore, implementing effective exercise programs in this population is challenging. Most individuals with MASLD fail to exercise regularly, citing time constraints, fatigue, pain, chronic health issues, lack of motivation, lack of enjoyment, and lack of education as the most commonly reported barriers [15, 16]. Thus, developing an exercise program that is acceptable to people with MASLD, is effective, and addresses these barriers, is essential to improving adherence and long-term sustainability.
While resistance exercises are effective, they often require specialized equipment and access to a gymnasium, which may limit accessibility and scalability. Eccentric exercise, which involves lengthening the muscle under tension, such as sitting to a chair slowly and descending stairs, has garnered attention due to its lower metabolic demand and reduced fatigue, potentially making it more suitable for individuals with MASLD [17, 18]. Compared to concentric training, eccentric exercise has been shown to produce greater increases in strength and muscle mass and to improve insulin sensitivity and lipid metabolism [19, 20].
Despite these advantages, only one study has investigated the effects of eccentric training on individuals with MASLD [21]. This study combined eccentric exercise with vitamin D supplementation in overweight women with MASLD and found significant reductions in liver enzymes alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT) and improvements in lipid profile. Therefore, the effects of eccentric training alone, particularly when delivered in a supervised, online, home-based format, appear to be an attractive intervention. This mode of delivery may help overcome common exercise barriers such as time constraints and travel limitations. Previous studies have demonstrated the benefits of resistance training in individuals with MASLD. For example, Takahashi et al [22] showed that simple resistance exercises, such as push-ups and squats, improved metabolic markers in this population. However, the intervention was delivered in-person and did not focus on eccentric contractions in the study. More broadly, a recent systematic review and meta-analysis by Zafar et al [23] reported that eHealth interventions, including mobile apps, telehealth, and web-based coaching, can improve liver enzymes and body composition in individuals with MASLD. While these findings support the feasibility of remote interventions, none of the included studies evaluated a fully supervised, real-time, bodyweight eccentric-only program tailored for this population. Given the physiological advantages and lower fatigue profile of eccentric exercise, its delivery in a digitally supervised, home-based format may offer a novel and accessible solution for overcoming common barriers to exercise in people with MASLD.
Therefore, the present study aimed to evaluate the effects of an 8-week online bodyweight eccentric exercise program on hepatic steatosis, liver enzymes, metabolic parameters, and physical function in patients with MASLD. We hypothesized that the intervention would be feasible and well-tolerated and would improve liver-related and metabolic health markers, whereas the control group receiving lifestyle advice would not demonstrate these changes.
| Materials and Methods | ▴Top |
Study design and participants
The present study was a pilot and feasibility quasi-randomized controlled trial which compared an online bodyweight eccentric exercise group with a non-exercise control group of individuals diagnosed with MASLD. This study was approved by the Human Research Ethics Committee of the South Metropolitan Health Service (RGS0000005982) and Edith Cowan University (2023-04727-DESHPANDE), and conducted in accordance with the Declarations of Helsinki and Istanbul. The trial was retrospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTR; Trial ID: ACTRN12626000100392).
We recruited adults (≥ 18 years) diagnosed with MASLD attending the hepatology outpatient clinic of a tertiary Australian hospital, identified during routine appointments based on hepatic steatosis or elevated liver enzymes. Consecutive patients were approached to minimize selection bias and improve generalizability. Participants underwent FibroScan® 502 Touch to assess hepatic steatosis severity using the controlled attenuation parameter (CAP) and liver fibrosis with transient elastography (TE), respectively, following evaluation by an experienced hepatologist. MASLD diagnosis was based on a recent multi-society consensus [24]. Since a CAP score above 275 dB/m indicates a significant accumulation of liver fat [25], individuals with a CAP score of 275 dB/m or higher were invited to participate in the present study.
Exclusion criteria included other liver diseases, such as autoimmune hepatitis, viral hepatitis or significant alcohol consumption, hepatic encephalopathy, ascites, esophageal varices, consumption of weight-loss drugs, bariatric surgery, and hepatocellular carcinoma (HCC). It was a requirement that the participants had not been doing any structured resistance and/or aerobic exercise within the last 6 months.
A priori sample size estimation was performed using G*Power (version 3.1.9.7). An effect size of 0.8 was selected to represent a large effect, based on Cohen’s conventional criteria and the expectation that this pilot study would primarily detect relatively large changes in key liver-related outcomes following the intervention. Using an alpha level of 0.05 and 80% power, the estimated minimum total sample size was 12 participants. Of 25 contacted patients, 20 consented. However, three participants were excluded resulting in 17 eligible participants. Due to the quasi-randomized design, group allocation was based on availability and preference. This approach was necessary to accommodate the practical constraints faced by the participants, such as scheduling conflicts and logistical issues, while still aiming to maintain a balance between groups. Ten participants entered the exercise group and seven the control group. One participant in the exercise group withdrew after 5 weeks due to personal reasons, leaving nine in the exercise group and seven in the control group. A per-protocol analysis was conducted on those who completed the intervention.
Among the 16 participants, there were equal numbers of men and women (n = 8 each). Table 1 summarizes baseline characteristics. The two groups were similar in age, sex, ethnicity, body mass index (BMI), steatosis grade, and fibrosis stage (P > 0.05), although more participants in the exercise group had T2DM (89% vs. 29%; P = 0.01).
 Click to view | Table 1. Baseline Characteristics of Participants in the Exercise and Control Groups |
Exercise intervention
A home-based online bodyweight eccentric exercise program was designed and supervised by the investigator in collaboration with an experienced exercise physiologist. Spanning over 8 weeks, the program consisted of five sessions per week, each progressing from 5 to 25 min. This gradual progression accommodated varying fitness levels and helped prevent participant overload. Each session began with a 5-min dynamic warm-up and ended with a 5-min static stretching cool-down for safety and recovery.
The exercises included chair squats, heel raises, abdominal reclines, and push-ups to target major muscle groups essential for functional mobility in older adults, as supported by previous studies [22, 26]. These exercises were selected based on prior study reporting their safety and suitability for individuals with metabolic and functional limitations [27]. The program followed a structured progression: week 1 involved one set of five reps per exercise; week 2, two sets of five; weeks 3–4, one set of ten; weeks 5–6, two sets of ten; and weeks 7–8, three sets of ten. The progression was structured to ensure gradual overload while accommodating individual tolerance.
The investigator accessed the participants through Google Meet invites, which allowed for real-time supervision throughout the sessions. To ensure a strong foundation for the exercises, participants received in-person instructions for the eccentric bodyweight exercises at the beginning of the study. During sessions, the investigator demonstrated movements, corrected techniques if necessary, and provided feedback. This real-time supervision enabled the investigator to closely observe the participants, offering immediate feedback on their forms and techniques. Moreover, the online format facilitated individualized support, as the investigator was able to address participants’ specific concerns and modify exercises as needed. The real-time supervision also allowed modification of exercises according to participant capability, as important component of process evaluation.
Control group participants received general lifestyle advice per European Association for the Study of the Liver (EASL) guidelines [28] and were offered the exercise program after study completion.
Primary and secondary outcome measures
Primary outcomes included changes in hepatic steatosis severity based on FibroScan® CAP scores, liver stiffness measurement (LSM), levels of AST, ALT, and GGT, blood glucose, glycosylated hemoglobin (HbA1c), insulin, low-density lipoprotein (LDL-C), high-density lipoprotein (HDL-C), total cholesterol (TC), and TG concentration in the blood. Participants fasted for at least 12 h before venesection and blood analysis at a nationally accredited diagnostic laboratory. Insulin resistance was assessed using the homeostasis model assessment insulin resistance (HOMA-IR) index calculation: HOMA-IR = fasting insulin × fasting blood glucose/22.5.
Secondary outcomes included BMI, waist circumference (WC), hip circumference, triglyceride glucose waist index (TyG-WC), fatty liver index (FLI), fibrosis-4 index (Fib-4), and physical function tests. Waist circumference was measured at the end of normal exhalation midway between the lowest rib and the top of the iliac crest, with the participant standing and relaxed. Hip circumference was measured at the widest part of the hips and buttocks at the end of exhalation in a relaxed stance.
The Fib-4 index was calculated using age, AST, ALT, and platelet levels [29]. FLI included BMI, WC, TG, and GGT levels, while TyG-WC was calculated using TG, fasting glucose, and WC [30]. Together, these tests offer a cost-effective, validated, and reliable means of noninvasively stratifying risk, monitoring progression, and informing treatment decisions in MASLD care. All assessments were conducted at baseline and after the 8-week intervention. Blood tests, CAP, and TE were performed after overnight fasting.
Physical function tests
The following physical function tests were performed only in the exercise group. These tests were chosen based on previous studies that assessed the effects of bodyweight eccentric exercise [23]. Physical function tests were not performed by the control group participants to avoid introducing a learning effect or unintentionally encouraging participation in physical activity, which could influence the comparability of outcomes. All tests were demonstrated to participants beforehand to ensure proper understanding of the movement patterns; however, a full familiarization trial was not conducted due to time and practical constraints. These assessments have strong test–retest reliability in adults, and therefore a single well-standardized trial was considered acceptable within the clinical context of this study.
30-s sit-to-stand test
To measure lower-body strength, participants were asked to stand up and sit down from a chair as many times as possible within 30 s. We counted each full stand and there was only one trial for each participant.
2-min step test
Aerobic endurance was assessed. The participants were instructed to march in place, lifting each knee to a specified height, for two full minutes. The number of times the right knee reached the target height was counted. This study was a single trial.
3-m timed up and go test
Functional mobility and balance were assessed. The participants started from a sitting position, stood up, walked 3 m, turned, walked 3 m back, and sat down. The researchers recorded the time required to complete the task. A trial was conducted for each participant.
Hand grip strength test
Grip strength was measured using a hand dynamometer as an indicator of the overall muscle strength. The participants were instructed to squeeze the dynamometer as hard as possible with each hand. Two trials were performed for each hand and the highest average score from both hands was recorded.
One-leg balance test
This test measures the balance, stability, and coordination. The participants were asked to stand on one leg of their choice for a maximum of 60 s without support. The time required to maintain balance was recorded. Two trials were performed for each leg and the best results were recorded.
Survey about the exercise program
After completing the 8-week program, participants completed a brief online questionnaire (Qualtrics) to share their opinions and experiences. The survey included questions on the program’s relevance, usefulness, enjoyment, perceived difficulty, and challenges related to the online format. Participants also selected their favorite aspects from pre-populated options. These responses provided insights into the program’s acceptability and feasibility.
Statistical analyses
Data were analyzed using IBM SPSS Statistics for Windows (Version 29.0. Armonk, NY, USA: IBM Corp). Normality and homogeneity were assessed using the Shapiro–Wilk and Levene tests, respectively. Baseline differences between groups were analyzed using the Mann–Whitney U test. Within-group changes after 8 weeks were assessed using the paired Student’s t-test and Wilcoxon signed-rank test. A significance level of P < 0.05 was used. Results are presented as mean ± standard deviation (SD) and range (lowest to highest value).
| Results | ▴Top |
Primary and secondary outcomes
Table 2 shows changes in the outcome measures from baseline to 8 weeks later for the exercise and control groups. The exercise group showed decreases (P < 0.05) in body mass, BMI, WC, and hip circumference, but these were not found in the control group. In the exercise group, CAP scores, GGT, TyG-WC index, and FLI decreased significantly over the 8-week period (P < 0.05), but no significant changes were observed in the control group. TG, HDL, LDL, glucose, insulin, HOMA-IR, and HbA1c did not show significant changes (all P > 0.05) from baseline to 8 weeks for both exercise and control groups.
Click to view | Table 2. Changes of Variables From Baseline to 8 Weeks Later for the Exercise (n = 9) and Control (n = 7) Groups |
Figure 1 shows the variability among participants for changes in some of the above measures from baseline to 8 weeks later. Large individual variability was evident in the percentage changes, indicating the presence of both responders and non-responders within the exercise group. Some participants experienced marked improvements, while others showed minimal or no changes, emphasizing the heterogeneous responses to the exercise intervention.
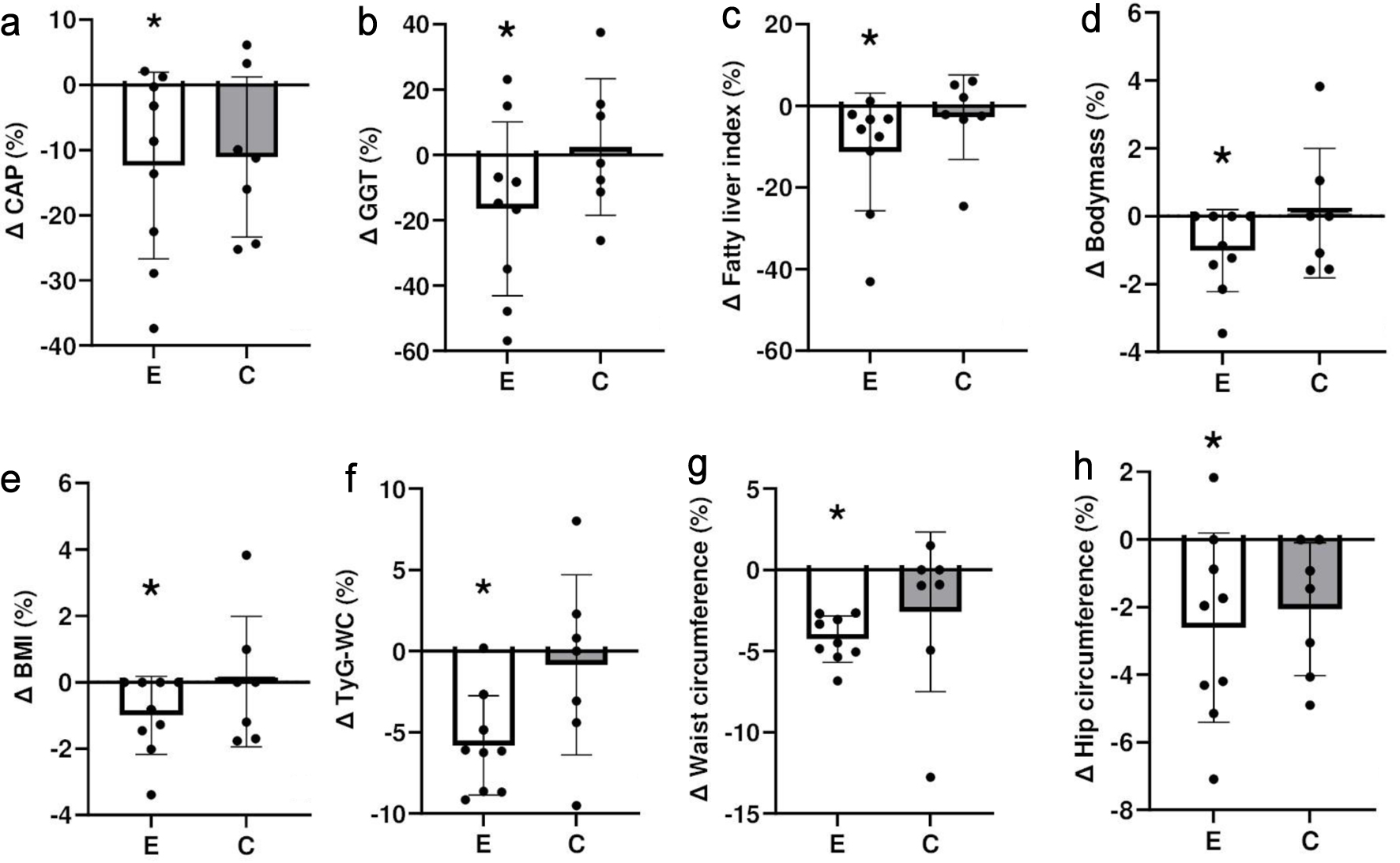 Click for large image | Figure 1. Comparison between exercise (E) and control (C) groups for percent changes in (a) controlled attenuation parameter (CAP), (b) gamma-glutamyl transferase (GGT) activity, (c) fatty liver index, (d) body mass, (e) body mass index (BMI), (f) triglyceride glucose waist index (TyG-WC), (g) waist circumference, and (h) hip circumference from baseline to 8 weeks later. *A statistically significant within-group change from baseline (P < 0.05). The figure illustrates group trends and inter-individual variability; formal between-group comparisons were not statistically significant. |
When comparing the exercise and control groups, CAP score decreased by 12% in the exercise group, GGT activity was reduced by 16%, FLI showed an 11% reduction in the exercise group, and TyG-WC demonstrated a decrease of 6% in the exercise group, but no significant changes were found in the control group. WC and hip circumference decreased by 4% and 3%, respectively, in the exercise group, while no significant changes were seen in the control group. Formal between-group comparisons did not show statistically significant differences, which is expected given the small sample size.
Physical fitness
As shown in Table 3, all physical fitness tests showed significant improvement after the exercise intervention. A large inter-individual variability was observed for the changes, but on average, the 2-min step count showed a 38% increase, the sit-to-stand repetition had a 26% increase, the balance test time increased 90%, and the 3-m timed up and go test time decreased by 15%.
Click to view | Table 3. Changes of Variables From Baseline to After 8-Week Training (Post-Training) for the Exercise Group |
Participant feedback
Participants in the exercise group were asked whether they would continue performing the exercises after the 8-week program had concluded, and 44% of the participants responded with “probably yes” or “definitely yes,” indicating a positive outlook on continuing the exercises. Seventy-eight percent of the participants found that the program was extremely relevant, 78% reported that the exercises were somewhat enjoyable, and 22% stated that the exercises were extremely enjoyable. In terms of difficulty, 44% of the participants found the exercises were not difficult to perform, 33% reported that the exercises were somewhat difficult, and 22% found the exercises somewhat difficult to perform. Importantly, 89% of participants did not find the online format difficult to follow, and the top three reasons for liking the program were that it was supervised by a professional, home-based, and no specialized equipment was required to perform the exercises.
| Discussion | ▴Top |
To the best of our knowledge, this was the first study to examine the effects of an online bodyweight eccentric exercise program on liver health, metabolic markers, and physical function in individuals with MASLD. The program was designed to address common barriers to exercise by offering a simple, structured, and low-fatigue solution requiring minimal equipment and time. All participants in the exercise group completed 40 sessions over 8 weeks, demonstrating high feasibility, acceptability, and adherence. The results supported the hypothesis that the exercise program would improve liver-related and metabolic health markers.
The exercise group demonstrated significant improvements in hepatic steatosis, WC, hip circumference (Table 2, Fig. 1), and physical fitness (Table 3) compared with baseline, with some notable improvements in liver enzymes and metabolic markers. These findings are consistent with previous studies supporting the effects of exercise on managing MASLD [13, 31]. Importantly, the present study uniquely employed a bodyweight, eccentric-only resistance training program delivered entirely online in real time. Eccentric exercise is metabolically less demanding and may be more suitable for individuals with MASLD who report fatigue, time constraints, or other comorbidities that limit traditional forms of exercise. The structured progression, live supervision, and real-time feedback likely contributed to the high adherence rate and effective engagement. The 100% adherence among those who completed the intervention suggests that this format may overcome common physical and psychological barriers, such as lack of motivation, pain, or lack of access to facilities. This aligns with previous research identifying these barriers as major obstacles for patients with MASLD [15]. The program’s home-based and supervised delivery model is also low-cost and scalable, offering a viable alternative to both gym-based exercise and expensive pharmacological interventions. Unlike medications that typically target advanced disease and may be financially inaccessible to many, this intervention requires no specialized equipment or infrastructure and could be delivered widely in clinical or community settings.
In the exercise group, hepatic steatosis measured by CAP decreased significantly over the 8-week intervention period. However, LSM, which reflects hepatic fibrosis rather than steatosis, did not change during the study period (Table 3). Previous studies reported mixed results regarding the effect of short-term exercise on liver stiffness. Some studies found a modest reduction in liver stiffness, whereas others suggested that longer intervention periods might be required to detect significant changes in fibrosis markers [32]. Oh et al [33] stated that only high-intensity aerobic exercise, but not moderate-intensity aerobic and resistance exercises, was effective in improving liver stiffness. The absence of change in LSM in this study may therefore be due to the short duration and the resistance-based nature of the program. Given the small sample size and quasi-randomized design, the observed reduction in CAP should be interpreted as exploratory and hypothesis-generating rather than definitive evidence of intervention efficacy.
Although glucose, insulin resistance, and lipid profiles did not change significantly, the exercise group showed meaningful reductions in WC and hip circumference (Table 3). Additionally, the present study found significant improvements in the TyG-WC and the FLI in the exercise group. These anthropometric measures and biomarkers are reliable indicators of metabolic health and are independently associated with the presence or risk of developing MASLD and other metabolic disorders [34, 35]. Reductions in central obesity, as represented by decreases in WC and hip circumference, are strongly associated with improved metabolic outcomes [36]. The reduction in WC and hip circumference aligns with previous studies that demonstrated exercise-induced improvements in body composition attributed to reductions in subcutaneous trunk fat and visceral fat [37, 38]. Although some studies have reported that resistance training could reduce visceral fat, the reduction was typically smaller compared to aerobic exercise and dietary interventions [39]. Reducing visceral fat and improving insulin sensitivity leads to better glycemic and lipid metabolism, which can help reduce liver fat accumulation and prevent its progression to fibrosis [40].
The absence of significant changes in glucose, insulin, HOMA-IR, and lipid profile may reflect the short duration of the intervention, the relatively low external load inherent to bodyweight eccentric exercise, and the high prevalence of T2DM in the exercise group. In individuals with long-standing metabolic dysfunction, improvements in glycemic or lipid measures often require longer intervention periods or higher training volumes. Therefore, the non-significant findings are not unexpected and should be interpreted within the context of the study design rather than as a lack of physiological benefit.
Improvements in FLI and TyG-WC also support the use of these indices as sensitive markers of metabolic health in MASLD populations [41–43]. Improvements in these indices suggest that the eccentric exercise program not only reduced liver fat but also improved other aspects of metabolic health. GGT is strongly associated with liver steatosis and metabolic dysfunction, and its reduction may signal a decrease in hepatic fat and oxidative stress [44]. Although changes in ALT and AST levels did not reach statistical significance, the trend towards improvement in these markers suggests the potential benefits of eccentric exercise.
There was considerable inter-individual variability in response to the intervention, as shown in Figure 1. While some participants showed marked improvements, others showed minimal or no change, despite adhering fully to the program. This heterogeneity is consistent with previous exercise trials [45] and may reflect differences in baseline health, lifestyle, motivation, or genetic predisposition. Such variability reinforces the need for personalized approaches to exercise prescription in MASLD management. Nonetheless, these improvements were not observed in the control group, suggesting that the intervention played a key role in driving these changes.
MASLD is associated with cardiovascular disease, which represents the leading cause of mortality in this population [46, 47]. Both conditions share common pathophysiological mechanisms including insulin resistance, systemic inflammation, endothelial dysfunction, and visceral adiposity. Consequently, improvements in metabolic health and central adiposity observed in the present study may have broader cardiometabolic implications beyond liver-specific outcomes. Regular exercise is known to improve endothelial function, reduce systemic inflammation, and enhance cardiometabolic health, which may partly explain the beneficial changes observed in the present study. Recent reviews have highlighted the bidirectional relationship between MASLD and cardiovascular disease and emphasize the importance of lifestyle interventions, particularly exercise, in improving both hepatic and cardiovascular risk profiles [46, 48].
The exercise group showed improvements across several physical function tests, including the 2-min step test, sit-to-stand test, single-leg balance test, and 3-m timed up and go test (Table 3). The gains indicate enhanced aerobic capacity, mobility, functional independence, muscular strength, and balance which are known benefits of eccentric training [19, 20]. Moreover, these benefits are especially important for individuals with MASLD, who often experience fatigue and reduced functional capacity. Grip strength did not improve, which is consistent with the training specificity principle. The program primarily targeted the lower body and trunk with only minimal direct loading of the forearm flexors. Additionally, several participants had T2DM, in whom reduced peripheral nerve function and handgrip responsiveness are common. Given the low absolute upper-limb training volume, minimal change in grip strength is expected and does not contradict the broader functional gains observed.
The beneficial effects observed may be partly explained by physiological mechanisms previously associated with eccentric exercise. However, because the study did not include a comparison exercise group, these improvements may not be attributed specifically to eccentric contractions and may instead reflect the general benefits of engaging in regular resistance exercise. Nonetheless, several eccentric-related mechanisms provide useful context for understanding the potential adaptations observed. Eccentric exercises are less metabolically demanding, as shown by lower oxygen consumption and heart rate for the same work in eccentric cycling than for concentric cycling [49]. This is likely to make them more tolerable for individuals with MASLD who experience fatigue [17]. Furthermore, eccentric contractions produce distinct neuromuscular responses such as enhanced central nervous activity, increased muscle-tendon stiffness, and increased muscle protein synthesis [50]. It also increases glucose transporter type 4 (GLUT4) translocation in skeletal muscle, facilitating glucose uptake independent of insulin, which may contribute to improved metabolic function [51]. Additionally, eccentric exercise stimulates the release of myokines like interleukin-6 (IL-6) and irisin, which reduce inflammation and promote lipid oxidation, potentially mitigating liver inflammation and fat storage [51]. The reductions in CAP and improvements in GGT observed in the present study may plausibly reflect improvements in insulin sensitivity, skeletal muscle glucose uptake, and myokine-mediated metabolic regulation induced by resistance exercise. While these mechanisms were not directly measured in this study, they are plausible contributors to the observed changes and warrant further investigation in future research.
Post-program feedback indicated that most participants found the exercises highly relevant, enjoyable, and easy to perform. The online format was well received, with participants highlighting the convenience of supervised, at-home sessions requiring no travel or equipment. These findings reinforce the potential of remote, supervised interventions to improve accessibility, especially in populations with low confidence, comorbidities, or logistical barriers to attending in-person programs. The ability to provide real-time feedback and modify exercises individually also supports safe implementation and high engagement.
The present study had several limitations. The small sample size and quasi-randomized design limit internal validity and generalizability. Future randomized controlled trials should incorporate formal power calculations to determine an adequate sample size capable of detecting clinically meaningful changes in hepatic and metabolic outcomes. Participants self-selected into the intervention or control group based on availability and preference, which may have introduced selection bias. Additionally, individuals who opted for the exercise group may have had greater motivation or readiness for lifestyle change, which could have influenced the observed outcomes independently of the intervention. The marked imbalance in T2DM prevalence between the groups may also have confounded metabolic outcomes, as diabetes is a major driver of MASLD progression and may influence responsiveness to lifestyle interventions. Future studies should consider stratified randomization by diabetes status and relevant medication use. However, this approach mirrors real-world conditions and improves ecological validity, as it reflects the choices patients typically make in clinical settings. The study duration was relatively short, and long-term sustainability of the observed benefits is unknown. Dietary intake was not monitored, which may have influenced metabolic markers. However, this was an intentional design choice to isolate the effects of the exercise intervention. The absence of muscle mass measurements is another limitation, given the known relationship between skeletal muscle and MASLD management via enhancing insulin sensitivity, lipid metabolism, and metabolic health [52]. Future studies should include dual-energy X-ray absorptiometry (DEXA) or bioelectrical impedance analysis (BIA) to assess changes in lean mass. Finally, while this online exercise program shows promise as a scalable intervention, it does not address barriers like internet access, digital literacy, or socioeconomic constraints. Physical function assessments were performed only in the exercise group; therefore, these improvements should be interpreted as within-group observations and not as definitive between-group intervention effects. Future studies should include these assessments in both groups.
Our findings align with recent evidence demonstrating the multi-system involvement of MASLD. A 2024 systematic review confirmed strong links between sarcopenia and MASLD progression, highlighting the importance of maintaining muscle function in this population [53]. In conclusion, this pilot study suggests that a supervised, online, home-based eccentric bodyweight exercise program is feasible, well tolerated, and associated with improvements in hepatic steatosis, central adiposity, and physical function in adults with MASLD. While the findings are encouraging, the small sample size and quasi-randomized design mean that the results should be interpreted as preliminary. Larger randomized controlled trials with adequate sample sizes and longer follow-up are needed to confirm the efficacy and long-term sustainability of this intervention.
Acknowledgments
The authors sincerely thank all the patients who participated in the study for their valuable time and effort. We also extend our gratitude to Fiona Stanley Hospital for providing the facilities and support necessary to conduct this study. Special thanks to the nursing staff for their assistance and dedication, which was instrumental in ensuring smooth execution of the study.
Financial Disclosure
This work was supported by a PhD scholarship from Edith Cowan University. The university did not have any role in the study design, data collection, analysis, or interpretation of the data, in writing this manuscript, or in the decision to submit the article for publication.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Written informed consent was obtained prior to participation.
Author Contributions
Substantial contributions to study concepts and design: KD, KN, OA, and JO. Acquisition of data: KD, OA, and AM. Analyses and interpretation of data: KD, KN, OA, and ISR. Drafting of the manuscript: KD. Statistical Analysis: KD. Figures and Tables: KD, KN, and OA. Critical revision of the manuscript for important intellectual content: KD, KN, JO, OA, and ISR.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ALT: alanine aminotransferase; AST: aspartate aminotransferase; BIA: bioelectrical impedance analysis; BMI: body mass index; CAP: controlled attenuation parameter; DEXA: dual-energy X-ray absorptiometry; EASL: European Association for the Study of the Liver; Fib-4: fibrosis-4 index; FLI: fatty liver index; GGT: gamma-glutamyl transferase; GLUT4: glucose transporter type 4; HbA1c: glycosylated hemoglobin; HCC: hepatocellular carcinoma; HDL: high-density lipoprotein; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; IL-6: interleukin-6; LDL: low-density lipoprotein; LDL-C: low-density lipoprotein cholesterol; LSM: liver stiffness measurement; MASH: metabolic dysfunction-associated steatohepatitis; MASLD: metabolic dysfunction-associated steatotic liver disease; NAFLD: non-alcoholic fatty liver disease; SD: standard deviation; SPSS: Statistical Package for the Social Sciences; T2DM: type 2 diabetes mellitus; TC: total cholesterol; TE: transient elastography; TG: triglyceride; TyG-WC: triglyceride glucose waist index; WC: waist circumference
| References | ▴Top |
- Rinella ME, Sookoian S. From NAFLD to MASLD: updated naming and diagnosis criteria for fatty liver disease. J Lipid Res. 2024;65(1):100485.
doi pubmed - Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335-1347.
doi pubmed - Maurice J, Manousou P. Non-alcoholic fatty liver disease. Clin Med (Lond). 2018;18(3):245-250.
doi pubmed - Issa G, Shang Y, Strandberg R, Hagstrom H, Wester A. Cause-specific mortality in 13,099 patients with metabolic dysfunction-associated steatotic liver disease in Sweden. J Hepatol. 2025;83(3):643-651.
doi pubmed - Younossi ZM, Kalligeros M, Henry L. Epidemiology of metabolic dysfunction-associated steatotic liver disease. Clin Mol Hepatol. 2025;31(Suppl):S32-S50.
doi pubmed - Ayonrinde OT, Olynyk JK, Beilin LJ, Mori TA, Pennell CE, de Klerk N, Oddy WH, et al. Gender-specific differences in adipose distribution and adipocytokines influence adolescent nonalcoholic fatty liver disease. Hepatology. 2011;53(3):800-809.
doi pubmed - Younossi ZM, Henry L. Understanding the burden of nonalcoholic fatty liver disease: time for action. Diabetes Spectr. 2024;37(1):9-19.
doi pubmed - Gastaldelli A, Cusi K. From NASH to diabetes and from diabetes to NASH: mechanisms and treatment options. JHEP Rep. 2019;1(4):312-328.
doi pubmed - Hagstrom H, Shang Y, Hegmar H, Nasr P. Natural history and progression of metabolic dysfunction-associated steatotic liver disease. Lancet Gastroenterol Hepatol. 2024;9(10):944-956.
doi pubmed - Cho HJ, Hwang S, Park JI, Yang MJ, Hwang JC, Yoo BM, Lee KM, et al. Improvement of nonalcoholic fatty liver disease reduces the risk of type 2 diabetes mellitus. Gut Liver. 2019;13(4):440-449.
doi pubmed - Oh YH, Jeong S, Park SJ, Ahn JC, Park SM. Reversal of nonalcoholic fatty liver disease reduces the risk of cardiovascular disease among Korean. Medicine (Baltimore). 2023;102(44):e35804.
doi pubmed - Romero-Gomez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. 2017;67(4):829-846.
doi pubmed - Hashida R, Kawaguchi T, Bekki M, Omoto M, Matsuse H, Nago T, Takano Y, et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: a systematic review. J Hepatol. 2017;66(1):142-152.
doi pubmed - Charatcharoenwitthaya P, Kuljiratitikal K, Aksornchanya O, Chaiyasoot K, Bandidniyamanon W, Charatcharoenwitthaya N. Moderate-intensity aerobic vs resistance exercise and dietary modification in patients with nonalcoholic fatty liver disease: a randomized clinical trial. Clin Transl Gastroenterol. 2021;12(3):e00316.
doi pubmed - Deshpande K, Olynyk J, Ayonrinde O, Nosaka K. Barriers to exercise in patients with metabolic dysfunction-associated steatotic liver disease: a patient survey. J Clin Med Res. 2024;16(2-3):94-105.
doi pubmed - Glass O, Liu D, Bechard E, Guy CD, Pendergast J, Mae Diehl A, Abdelmalek MF. Perceptions of exercise and its challenges in patients with nonalcoholic fatty liver disease: a survey-based study. Hepatol Commun. 2022;6(2):334-344.
doi pubmed - Szucs G, Pipicz M, Szabo MR, Csont T, Torok L, Csonka C. Effect of eccentric exercise on metabolic health in diabetes and obesity. Sports Med Open. 2023;9(1):91.
doi pubmed - Julian V, Thivel D, Costes F, Touron J, Boirie Y, Pereira B, Perrault H, et al. Eccentric training improves body composition by inducing mechanical and metabolic adaptations: a promising approach for overweight and obese individuals. Front Physiol. 2018;9:1013.
doi pubmed - Chen TC, Hsieh CC, Tseng KW, Ho CC, Nosaka K. Effects of Descending Stair Walking on Health and Fitness of Elderly Obese Women. Med Sci Sports Exerc. 2017;49(8):1614-1622.
doi pubmed - Chen TC, Tseng WC, Huang GL, Chen HL, Tseng KW, Nosaka K. Superior effects of eccentric to concentric knee extensor resistance training on physical fitness, insulin sensitivity and lipid profiles of elderly men. Front Physiol. 2017;8:209.
doi pubmed - Rahimpour Z, Hoseini R, Behpour N. Alterations of liver enzymes and lipid profile in response to exhaustive eccentric exercise: vitamin D supplementation trial in overweight females with non-alcoholic fatty liver disease. BMC Gastroenterol. 2022;22(1):372.
doi pubmed - Takahashi A, Abe K, Usami K, Imaizumi H, Hayashi M, Okai K, Kanno Y, et al. Simple resistance exercise helps patients with non-alcoholic fatty liver disease. Int J Sports Med. 2015;36(10):848-852.
doi pubmed - Zafar Y, Sohail MU, Saad M, Ahmed SZ, Sohail MO, Zafar J, Lirette S, et al. eHealth interventions and patients with metabolic dysfunction-associated steatotic liver disease: a systematic review and meta-analysis. BMJ Open Gastroenterol. 2025;12(1):e001670.
doi pubmed - Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, Romero D, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542-1556.
doi pubmed - Cao YT, Xiang LL, Qi F, Zhang YJ, Chen Y, Zhou XQ. Accuracy of controlled attenuation parameter (CAP) and liver stiffness measurement (LSM) for assessing steatosis and fibrosis in non-alcoholic fatty liver disease: A systematic review and meta-analysis. EClinicalMedicine. 2022;51:101547.
doi pubmed - Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, Ryan ED. Resistance training for older adults: position statement from the national strength and conditioning association. J Strength Cond Res. 2019;33(8):2019-2052.
doi pubmed - Katsura Y, Takeda N, Hara T, Takahashi S, Nosaka K. Comparison between eccentric and concentric resistance exercise training without equipment for changes in muscle strength and functional fitness of older adults. Eur J Appl Physiol. 2019;119(7):1581-1590.
doi pubmed - European Association for the Study of the Liver, European Association for the Study of Diabetes, European Association for the Study of Obesity. EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388-1402.
doi pubmed - Vieira Barbosa J, Milligan S, Frick A, Broestl J, Younossi Z, Afdhal NH, Lai M. Fibrosis-4 index as an independent predictor of mortality and liver-related outcomes in NAFLD. Hepatol Commun. 2022;6(4):765-779.
doi pubmed - Ho B, Thompson A, Jorgensen AL, Pirmohamed M. Role of fatty liver index in risk-stratifying comorbid disease outcomes in non-alcoholic fatty liver disease. JHEP Rep. 2023;5(12):100896.
doi pubmed - Thorp A, Stine JG. Exercise as medicine: the impact of exercise training on nonalcoholic fatty liver disease. Curr Hepatol Rep. 2020;19(4):402-411.
doi pubmed - Oh S, Tsujimoto T, Kim B, Uchida F, Suzuki H, Iizumi S, Isobe T, et al. Weight-loss-independent benefits of exercise on liver steatosis and stiffness in Japanese men with NAFLD. JHEP Rep. 2021;3(3):100253.
doi pubmed - Oh S, So R, Shida T, Matsuo T, Kim B, Akiyama K, Isobe T, et al. High-intensity aerobic exercise improves both hepatic fat content and stiffness in sedentary obese men with nonalcoholic fatty liver disease. Sci Rep. 2017;7:43029.
doi pubmed - Danielsson O, Nissinen MJ, Jula A, Salomaa V, Mannisto S, Lundqvist A, Perola M, et al. Waist and hip circumference are independently associated with the risk of liver disease in population-based studies. Liver Int. 2021;41(12):2903-2913.
doi pubmed - Li S, Feng L, Ding J, Zhou W, Yuan T, Mao J. Triglyceride glucose-waist circumference: the optimum index to screen nonalcoholic fatty liver disease in non-obese adults. BMC Gastroenterol. 2023;23(1):376.
doi pubmed - Jayedi A, Soltani S, Zargar MS, Khan TA, Shab-Bidar S. Central fatness and risk of all cause mortality: systematic review and dose-response meta-analysis of 72 prospective cohort studies. BMJ. 2020;370:m3324.
doi pubmed - Abdelbasset WK, Tantawy SA, Kamel DM, Alqahtani BA, Soliman GS. A randomized controlled trial on the effectiveness of 8-week high-intensity interval exercise on intrahepatic triglycerides, visceral lipids, and health-related quality of life in diabetic obese patients with nonalcoholic fatty liver disease. Medicine (Baltimore). 2019;98(12):e14918.
doi pubmed - Damor K, et al. Effect of progressive resistance exercise training on hepatic fat in Asian Indians with non-alcoholic fatty liver disease. Journal of Advances in Medicine and Medical Research. 2013;4(1):114-124.
- Khalafi M, Malandish A, Rosenkranz SK, Ravasi AA. Effect of resistance training with and without caloric restriction on visceral fat: A systemic review and meta-analysis. Obes Rev. 2021;22(9):e13275.
doi pubmed - Bansal S, et al. Visceral fat: a key mediator of NAFLD development and progression. Human Nutrition & Metabolism. 2023;33:200210.
- Motamed N, Faraji AH, Khonsari MR, Maadi M, Tameshkel FS, Keyvani H, Ajdarkosh H, et al. Fatty liver index (FLI) and prediction of new cases of non-alcoholic fatty liver disease: A population-based study of northern Iran. Clin Nutr. 2020;39(2):468-474.
doi pubmed - Khamseh ME, Malek M, Abbasi R, Taheri H, Lahouti M, Alaei-Shahmiri F. Triglyceride glucose index and related parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) identify nonalcoholic fatty liver and liver fibrosis in individuals with overweight/obesity. Metab Syndr Relat Disord. 2021;19(3):167-173.
doi pubmed - Contreras D, Gonzalez-Rocha A, Clark P, Barquera S, Denova-Gutierrez E. Diagnostic accuracy of blood biomarkers and non-invasive scores for the diagnosis of NAFLD and NASH: Systematic review and meta-analysis. Ann Hepatol. 2023;28(1):100873.
doi pubmed - Chen LW, Huang MS, Shyu YC, Chien RN. Gamma-glutamyl transpeptidase elevation is associated with metabolic syndrome, hepatic steatosis, and fibrosis in patients with nonalcoholic fatty liver disease: A community-based cross-sectional study. Kaohsiung J Med Sci. 2021;37(9):819-827.
doi pubmed - Keating SE, Hackett DA, Parker HM, O'Connor HT, Gerofi JA, Sainsbury A, Baker MK, et al. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J Hepatol. 2015;63(1):174-182.
doi pubmed - Suresh MG, Mohamed S, Geetha HS, Prabhu S, Trivedi N, Mehta PD, Damodaran UK, et al. Cardiovascular implications in metabolic dysfunction-associated steatotic liver disease (MASLD): a State-of-the-Art Review. Korean Circ J. 2026;56(2):103-130.
doi pubmed - Goodheart RH, Ayonrinde OT. Connecting the dots: hepatic steatosis as a central player in the choreography of the liver-cardiovascular-kidney-metabolic syndrome. Heart Lung Circ. 2025;34(10):1050-1059.
doi pubmed - Brar AS, Khanna T, Sohal A, Hatwal J, Sharma V, Singh C, Batta A, et al. Metabolic dysfunction-associated steatotic liver disease and heart failure with preserved ejection fraction: A state-of-the-art review. World J Cardiol. 2026;18(1):111954.
doi pubmed - Penailillo L, Blazevich AJ, Nosaka K. Factors contributing to lower metabolic demand of eccentric compared with concentric cycling. J Appl Physiol (1985). 2017;123(4):884-893.
doi pubmed - Hody S, Croisier JL, Bury T, Rogister B, Leprince P. Eccentric muscle contractions: risks and benefits. Front Physiol. 2019;10:536.
doi pubmed - Ho CT, Otaka M, Kuo CH. Improving glucose tolerance by muscle-damaging exercise. J Tradit Complement Med. 2017;7(2):141-144.
doi pubmed - Kim G, Lee SE, Lee YB, Jun JE, Ahn J, Bae JC, Jin SM, et al. Relationship between relative skeletal muscle mass and nonalcoholic fatty liver disease: a 7-year longitudinal study. Hepatology. 2018;68(5):1755-1768.
doi pubmed - Malik A, Javaid S, Malik MI, Qureshi S. Relationship between sarcopenia and metabolic dysfunction-associated steatotic liver disease (MASLD): A systematic review and meta-analysis. Ann Hepatol. 2024;29(6):101544.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.