Risk Stratification and Contemporary Predictors of Survival in Hepatocellular Carcinoma Treated With Transarterial Radioembolization
DOI:
https://doi.org/10.14740/gr2049Keywords:
Risk stratification, Hepatocellular carcinoma, Transarterial radioembolization, TARE, Liver function, Y90Abstract
Background: Identifying risk factors for poor outcomes in patients with hepatocellular carcinoma (HCC) treated with transarterial radioembolization (TARE) can aid in developing personalized management strategies, such as the early use of immune checkpoint inhibitors (ICIs).
Methods: In this retrospective review, we included HCC patients who received TARE at The Ohio State University Comprehensive Cancer Center from January 1, 2015, to August 30, 2022. The Kaplan-Meier method was used to estimate progression-free survival (PFS) and overall survival (OS). Cox proportional hazard analysis was conducted to find the independent predictors of PFS and OS.
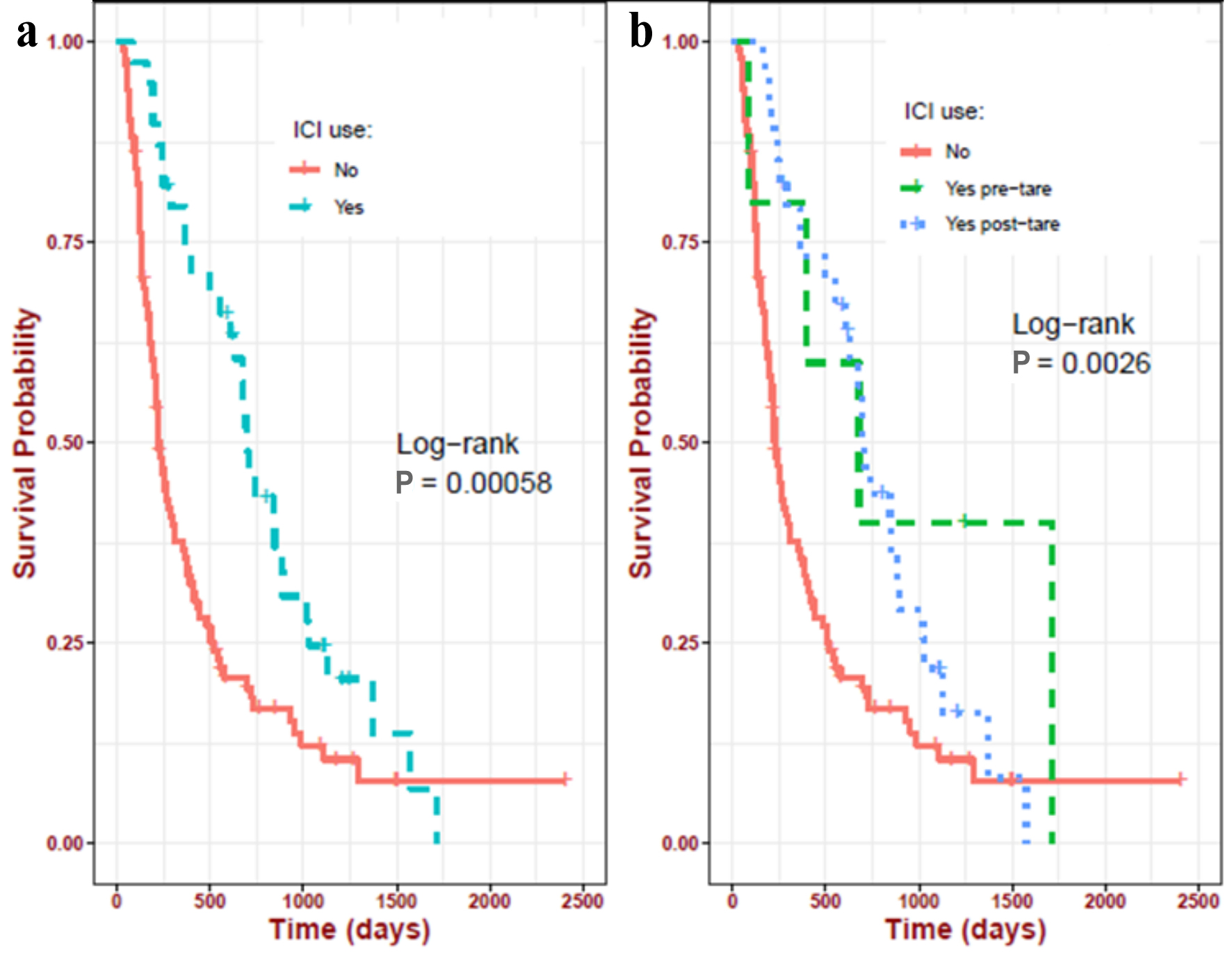
Results: We included 141 patients (median age of 65 years; 80% Caucasian; 80% male). Better PFS was associated with higher albumin (alb) (hazard ratio (HR) = 0.58, P = 0.005) and lower total bilirubin (T bili) levels (HR = 0.70, P = 0.034). Better OS was associated with a history of ablation (HR = 0.35, P < 0.001) and higher pre-TARE alb (HR = 0.63, P = 0.01); OS was worse in those with hepatic encephalopathy (HR = 2.01, P = 0.006). There was a notable trend toward worse OS in patients with ascites (HR = 1.71, P = 0.06) and metabolic-dysfunction-associated fatty liver disease (MAFLD)-associated HCC (HR = 1.86, P = 0.08). The receipt of ICI therapy was associated with a significantly better OS (P = 0.016), with a median OS of 1,102 days (95% confidence interval (CI): 884 - 1,509) compared to 614 days (95% CI: 493 - 829).
Conclusion: We present pretreatment risk factors (low alb, high T bili, MAFLD, hepatic encephalopathy, and ascites) that can predict poor outcomes in HCC patients treated with TARE. Preemptively treating such high-risk patients with ICI could improve their outcomes.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.